More than 14 million people in the United Kingdom (UK) are currently living in poverty, and the number of people experiencing deep poverty is increasing (Joseph Rowntree Foundation, 2024).
In this report, we examine how experiences of poverty stigma are related to mental health outcomes in the UK. Our aim was to understand the impact of poverty stigma and who is most affected in order to inform solutions.

We addressed the following questions:
- Which groups are more likely to experience poverty stigma?
- Are particular types of service use associated with higher levels of poverty stigma?
- Which forms of poverty stigma are most strongly associated with mental health outcomes?
Read the report or download as a PDF below.
Authors: Greig Inglis, Edward Sosu, Fiona McHardy, Isabel Witteveen, Pamela Jenkins, Jo Finlay, Lee Knifton and Shari McDaid

Research funding by the Mental Health Foundation
Contents
Summary points
- Certain groups experiencing financial hardship are more likely to experience poverty stigma, such as benefits recipients and foodbank users.
- Experiences of poverty stigma are associated with greater levels of anxiety and depression.
What happens next?
- Anti-stigma interventions are needed to challenge negative attitudes and reduce individuals' exposure to poverty stigma.
- Service providers should consider how services are perceived by people on low incomes and how these services can challenge poverty stigma.
Background
More than 14 million people in the United Kingdom (UK) are currently living in poverty, and the number of people experiencing deep poverty is increasing (Joseph Rowntree Foundation, 2024). Poverty is a major cause of mental ill-health (Knifton and Inglis, 2020). This is because people living in poverty are more likely to experience stressful situations such as financial instability, inadequate housing and food insecurity that lead to anxiety and depression (Brisson et al., 2020).
There is increasing recognition amongst policy makers of the impact that poverty stigma can have on communities. For example, the Scottish Parliament’s Cross Party Group on Poverty launched an inquiry into the causes and consequences of poverty stigma in January 2022 (McLean, 2023). Stigma occurs when individuals are labelled as being different and are subsequently subjected to negative stereotypes and discrimination (Hatzenbuehler et al., 2013).
Previous qualitative research in the UK and internationally has documented how people living on low incomes experience various forms of mistreatment, rejection, and exclusion from other people as well as institutions such as social security services (Inglis et al., 2019). Our recent systematic review also found evidence, predominantly from qualitative studies, that experiences of poverty stigma are associated with a range of mental health and well-being outcomes (Inglis et al., 2023).
We build on this existing research here by quantitatively examining how experiences of poverty stigma are related to mental health outcomes in the UK. Our aim was to understand the impact of poverty stigma and who is most affected in order to inform solutions.
We addressed the following questions:
- Which groups are more likely to experience poverty stigma?
- Are particular types of service use associated with higher levels of poverty stigma?
- Which forms of poverty stigma are most strongly associated with mental health outcomes?
Methods
An online survey was conducted of 1,000 adults living in the UK. The survey was administered through Prolific.com and was issued to individuals who reported a household income of £30,000 or less.
In total, 962 respondents completed the survey and were included in the analysis. The majority of respondents lived in England (84%), followed by Scotland (9%), Wales (6%), and Northern Ireland (1%), and most respondents (71%) reported that they were “just about getting by” or finding it difficult financially.
Survey respondents were asked to complete a questionnaire on experiences of poverty stigma that was coproduced through feedback from people who had lived experience of poverty. The specific survey items relating to poverty stigma are provided in Appendix 1.
The survey also contained questions on participants’ subjective social status, food security and foodbank use, financial hardship, benefits receipt, and use of money advice or debt services. Participants also completed various measures of mental health and well-being, including the four item Patient Health Questionnaire (PHQ-4; Kroenke et al., 2009) which measures symptoms of anxiety and depression.
What we found
We found two main types of poverty stigma reported by the survey respondents. The first type of stigma was personal experiences of discrimination and unfair treatment from others due to living on a low income. We called this type of stigma
“received poverty stigma”.
Overall, 21% of all survey respondents reported that they had personally experienced at least one form of received poverty stigma “often” or “very often” in the past 12 months. This figure increased to 26% amongst respondents who reported that they were financially “just about getting by” or worse.
The second type of stigma was respondents’ beliefs that people living on low incomes are treated unfairly by decision makers and institutions, such as public services and the media.
We called this type of stigma “perceived structural stigma”. Overall, 82% of all survey respondents believed that people on low incomes experience at least one type of structural stigma “often” or “very often”. This figure increased to 85% amongst respondents who reported that they were financially “just about getting by” or worse.

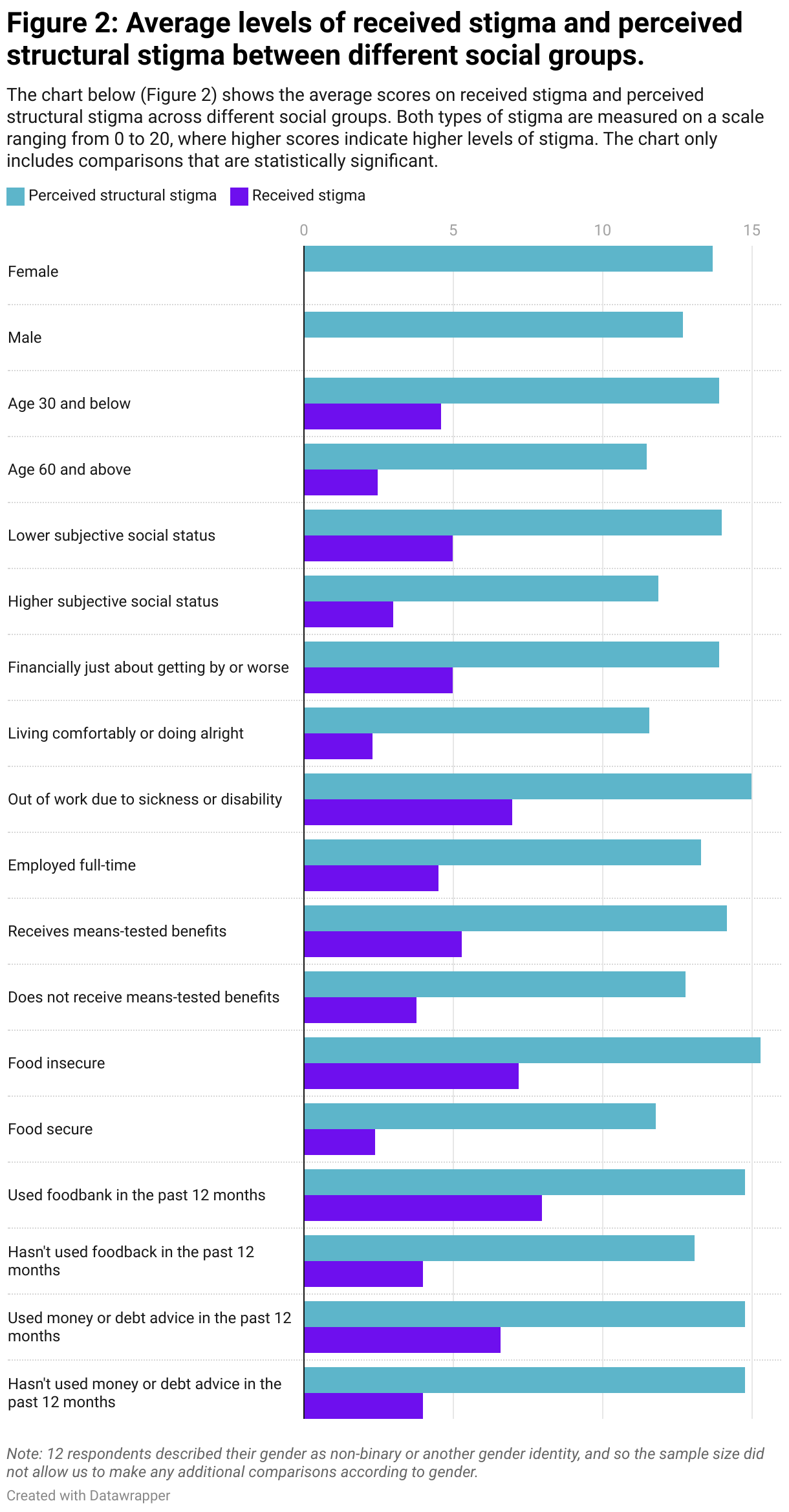
Which groups are more likely to experience poverty stigma?
Several groups were found to report higher levels of both received and perceived structural poverty stigma, including people who:
- were relatively young
- were financially just about getting by or worse
- rated their subjective social status as being relatively low
- were out of work due to sickness or disability
- received means tested benefits
- experienced food insecurity.
We also found that women reported higher levels of perceived structural stigma compared to men, although there were no gender differences in reports of received stigma.
There were also no differences in either received or perceived structural stigma between respondents who reported their ethnicity as white compared to all other ethnic groups combined, although the sample size was too small to examine differences between specific ethnic minority groups.
The differences highlighted above are also displayed in Appendix 2.
Are particular types of service use associated with higher levels of poverty stigma?
We also found that survey respondents who had used food banks in the past 12 months reported higher levels of both types of poverty stigma, as did respondents who had used money or debt advice services in the past 12 months.
Which forms of poverty stigma are most strongly associated with different mental health outcomes?
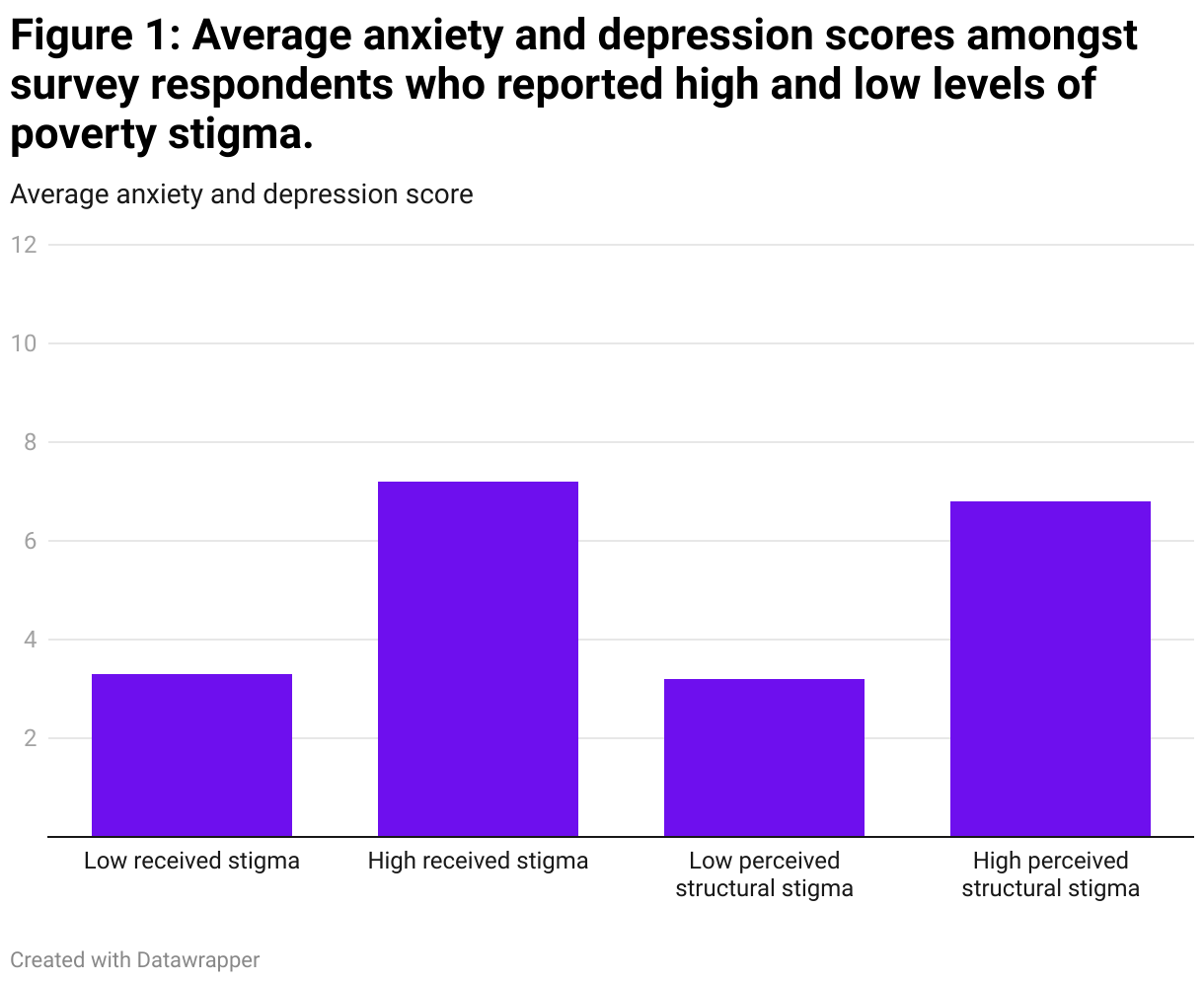
Experiences of both received stigma and perceived structural stigma were both positively associated with symptoms of anxiety and depression, even after accounting for experiences of financial hardship.
In other words, participants who reported higher levels of poverty stigma also reported higher levels of mental ill-health irrespective of the level of economic hardship experienced.
The relationship between experiences of poverty stigma and mental health is displayed in Figure 1. This chart shows the average levels of anxiety and depression amongst respondents who reported low and high levels of both types of stigma, with anxiety and depression measured on a scale ranging from 0 to 12.
Conclusion
In a survey of 1,000 UK adults with predominantly lower incomes, we found that experiences of poverty stigma were relatively common. Approximately one in five respondents reported that they had often experienced some type of discrimination or unfair treatment in the last 12 months because they live on a low income. Moreover, some groups were more likely to report poverty stigma, particularly those experiencing higher levels of financial hardship.
We also found that experiences of received stigma and perceived structural stigma are both positively associated with greater levels of anxiety and depression. While we can’t be sure that poverty stigma causes these poor mental health outcomes directly, addressing the sources of poverty stigma across society may be one approach to reduce socioeconomic inequalities in mental health.
Implications for policy and practice
- Challenging negative attitudes through anti-stigma interventions is a promising avenue for reducing individuals’ exposure
to received poverty stigma. Future interventions to challenge stigma should draw on learning from other types of antistigma campaigns such as those for mental health stigma. - Service providers should evaluate how services are perceived by people living on low incomes to ensure that service delivery does not contribute to perceptions of stigma.
- Social security systems in particular should examine how they can contribute to reducing poverty stigma through service
design and delivery. - Measures to address poverty stigma should include targeted action for higher risk groups.
- Measures of poverty stigma should be included as outcome measures in service evaluations.
- Measures of poverty stigma should be included in national surveys to monitor how experiences of stigma change over time and in response to changes in social policy.
It is important to note that the survey sample was not representative of the UK population, and as such we cannot make an accurate estimate of how many individuals experience poverty stigma among the general public. In addition, we are unable to determine whether experiences of stigma have a direct causal impact on mental health outcomes.
It is also important to note that poverty itself remains an important cause of mental ill-health, irrespective of how often individuals experience poverty stigma. As such, in addition to addressing stigma, it is also crucial to address economic difficulties faced by households and tackle poverty directly.
Brisson, D., McCune, S., Wilson, J. H., Speer, S. R., McCrae, J. S., & Hoops Calhoun, K. (2020). A systematic review of the association between poverty and biomarkers of toxic stress. Journal of Evidence-Based Social Work, 17, 696-713.
Hatzenbuehler, M. L., Phelan, J. C., & Link, B. G. (2013). Stigma as a fundamental cause of population health inequalities. American Journal of Public Health, 103, 813–821
Inglis, G., McHardy, F., Sosu, E., McAteer, J., & Biggs, H. (2019). Health inequality implications from a qualitative study of experiences of poverty stigma in Scotland. Social Science & Medicine, 232, 43-49.
Inglis, G., Jenkins, P., McHardy, F., Sosu, E., & Wilson, C. (2023). Poverty stigma, mental health, and well-being: A rapid review and synthesis of quantitative and qualitative research. Journal of Community & Applied Social Psychology, 33, 783-806.
Joseph Rowntree Foundation (2024). UK Poverty 2024. The essential guide to understanding poverty in the UK. Joseph Rowntree Foundation. https://www.jrf.org.uk/uk-poverty-2024-the-essential-guide-to-understanding-poverty-in-the-uk
Knifton, L., and Inglis, G. (2020). Poverty and mental health: policy, practice and research implications. BJPsych Bulletin, 44, 193-196.
Kroenke, K., Spitzer, R. L., Williams, J. B., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: the PHQ–4. Psychosomatics, 50, 613-621.
McLean, A. (2023). An inquiry into poverty-related stigma in Scotland. Poverty Alliance. https://www.povertyalliance.org/cross-party-group-on-poverty-report-ofinquiry-
into-poverty-related-stigma-in-scotland/
Appendix 1
Received stigma and perceived structural stigma were measured using two sets of five survey items. Respondents were asked to rate each item based on their experiences over the past 12 months using a scale ranging from 0 (never) to 4 (very often). Responses to both sets of items were them summed to create total scores for received stigma and perceived structural stigma.
Received stigma items:
- People have made negative assumptions about me because I don’t have much money.
- People have treated me badly because I don’t have much money.
- People have spoken down to me because I don’t have much money.
- People have blamed me because I don’t have much money.
- Family or friends have excluded me from things because I don’t have much money.
Perceived structural stigma items:
- People on low incomes are looked down on by television programmes in this country.
- People on low incomes in this country receive a lower standard of public services.
- Public services in this country make you feel inadequate when you are living on a low income.
- Politicians in this country look down on people who live on low incomes.
- People on low incomes are looked down on by newspapers in this country.
Related content
Mental health and the cost-of-living crisis report: another pandemic in the making?
We can't ignore the potentially devastating effect the cost-of-living crisis has on mental health. In this briefing paper we give an overview of the crisis's current and likely effects on people’s mental health.
Cost-of-living and mental health
Find out more about what you can do to protect your mental, emotional and physical health during the cost-of-living crisis and how you can help support others.